PIERRE BARBET
REVISITED
Frederick
T. Zugibe, M. D., Ph. D.
Adjunct Associate Professor of Pathology,
Columbia University, College of Physicians & Surgeons, N.Y.
Chief Medical Examiner, Rockland County, N.Y.
Reprinted
from Sindon N. S., Quad. No. 8, December 1995
Copyright 1995 - All Rights Reserved
Reprinted by permission.
(Illustrations have been added to the Internet version of this paper to aid the
viewer)
Introduction
There is no doubt that Dr. Pierre Barbet was a great pioneer in the field of
crucifixion and Shroud research and made major contributions in attempting to
collate the mechanisms of crucifixion with the findings on the Shroud.
1, 2 He is also one of the most widely quoted scientists in
crucifixion research but unfortunately, these quotes from Barbet's studies are
frequently misinterpreted as unqualified, proven facts instead of theories that
require confirmation by valid scientific studies that might challenge the
validity of his studies. Many medical articles have been written but are
entirely speculative and devoid of experimental studies. Many scientists
frequently forget that it is their duty, whenever possible, to provide
experimental support for their hypotheses. Father Weyland, the noted religious
sculptor, summed this up most aptly, "Conjectures and theories not backed up by
realistic experiments have always left me cold."
Barbet's studies are centered around three major hypotheses:
- The man of the Shroud of Turin was nailed through an area
of the wrist called Destot's Space and not through the palm of the hand.
- The missing thumb on the Shroud was due to injury to the
median nerve by the passage of the nail.
- The man of the Shroud died of asphyxiation.
It is the purpose of this paper to demonstrate that all three hypotheses
of Barbet are, in fact, untenable.
Hypothesis One
The man of the Shroud was nailed through the area of the wrist called
Destot's Space and not through the palm of the hand. When Barbet passed
nails through the middle of the palms of freshly amputated hands and found that
they tore through the skin between the fingers at a pull of about 88 pounds, he
collated this with mathematical calculations which revealed that if the body is
suspended with the arms at an angle of about 68 degrees with the upright there
is a pull on each hand greater than the entire weight of the body. He then
looked for a stronger area and following some experimentations he reported that
"...... one finds that in the middle of the bones of the wrists, there is a free
space bounded by the CAPITATE, the SEMILUNAR, the TRIQUETRAL
and the HAMATE bones. We know this space so well that we know in
accordance with DESTOT'S work.2
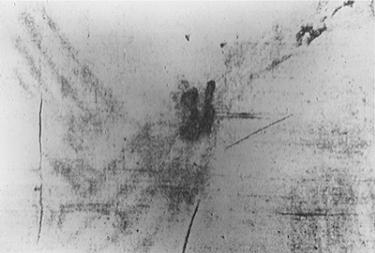
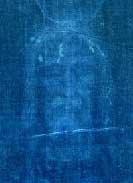
Figure 1
Unfortunately, THIS CANNOT BE TRUE because these four bones are
located on the little finger (ulnar) side of the wrist not on the thumb (radial)
side of the wrist as is depicted on the Shroud! LOOK AT THE HAND WOUND IMAGE
ON THE SHROUD TO CONFIRM THIS! Fig. 1) Note that the hand wound
image on the Shroud is indeed on the radial (thumb) side of the wrist.
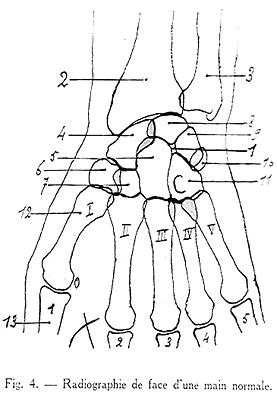
Figure 2
COULD BARBET HAVE JUST MADE AN ERROR IN NAMING THE BONES OF THE WRIST?
The answer is NO! because of the following: first of all, IN BARBET'S
1937 book, 1 the diagram of DESTOT'S SPACE (Fig.2)
unquestionably shows this space on the ulnar (little finger) side
of the wrist and NOT on the radial (thumb) side of
the wrist where the wound image is depicted on the Shroud. This is confirmed in
any anatomy text book.

Figure 3
Secondly, in the same book there is a photograph of a cadaver
that Barbet nailed to a cross which also shows that the nails are indeed nailed
through the small finger (ulnar) side of the wrist and not on the
thumb (radial) side (Fig. 3).
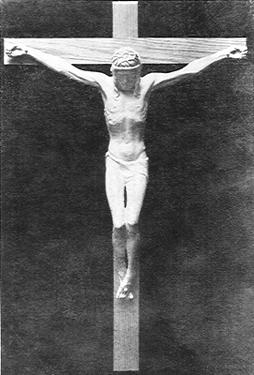
Figure 4
Thirdly, Barbet requested that Villandre, the master sculptor,
make a crucifix according to the "precise information" he had given him. This
was accomplished to Barbet's complete satisfaction. 1, 2 Again
note that the nail is in the small finger side of the wrist (Fig.4).
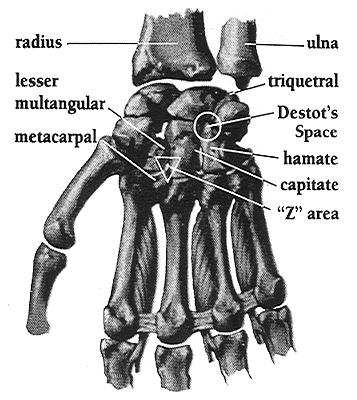
Figure 5
BARBET CONTINUED HIS CONFUSION AND MADE ANOTHER SERIOUS ANATOMICAL ERROR.
He said that when he drove the nail through Destot's Space, anywhere from 1/2 to
2/3 of the trunk of the median nerve was severed. This IS NOT
anatomically possible because the median nerve is not present in the area of
Destot's Space but instead runs along the wrist on the thumb (radial)
side of the wrist and along the thenar furrow into the palm of the hand. An easy
way to locate the median nerve on your own wrist is to bend your wrist forward.
You will see a firm, rope-like structure jutting outward. This is the palmaris
longus tendon which tells us that the median nerve runs along the thumb side of
this tendon. Obviously, Barbet was damaging the ulnar nerve which runs in
the area of Destot's space.
WHERE THEN WOULD THE WOUND HAVE TO BE MADE TO BE CONSISTENT WITH THE
SHROUD? Before answering this question, REMEMBER- the hand wound
image is located on the back of the hand and only depicts the EXIT of the
nail not its ENTRANCE. WE DON'T SPECIFICALLY KNOW WHERE THE NAIL ENTERED!

Figure 6
First of all, it can't be Destot's space because it's on the
wrong side of the wrist and,
Secondly, it can't be the center of the palm because it would not exit at
the site of the wound image where the Shroud shows it nor could it support the
weight of the body as determined by Barbet's experiments, and by mathematical
calculations.
Thirdly, it can't be the space between the radius and ulna because it
wouldn't exit where the Shroud shows it.

Figure 7
THIS LEAVES ONLY TWO POSSIBILITIES:
ONE: The thumb (radial) side of the wrist i.e. the area
of the wrist opposite Destot's Area. The nail could pass through the
radial (thumb) side of the wrist through a space created by four other carpal
bones; the NAVICULAR, LUNATE, GREATER MULTANGULAR and
CAPITATE bones, emerging where the Shroud depicts it. This is a very strong
area and the trunk of the median nerve would most likely be damaged by this
path.
TWO: The upper part of the palm of the hand ... NOT THE MIDDLE OF THE
PALM. This area is equally as sturdy as either Destot's Space or the radial
area indicated above and would emerge at the site depicted on the Shroud. This
area is located as follows; touch your thumb to the tip of your little finger. A
deep furrow called the thenar furrow is seen at the base of the bulky prominence
extending from the base of the thumb. This area was first pointed out by
Monsignor Alfonso Paleotto, Archbishop of Bologna, who accompanied St. Charles
Borromeo to Turin in 1598. It may be of interest that he postulated that the
nail would have entered the upper part of the palm obliquely, and pointing
toward the arm, it would have emerged where the Shroud depicts it. It is of
interest that Barbet severely criticized Paleotto's hypothesis as "anatomically
impossible." Monsignor Paleotto was indeed correct. If a nail is driven into
this furrow, a few centimeters from where the furrow begins at the wrist, with
the point of the nail angled at ten to fifteen degrees toward the wrist and
slightly toward the thumb, there is a natural inclination of the nail to an area
created by the METACARPAL bone of the index finger and the
CAPITATE and LESSER MULTANGULAR bones of the wrist
which we have coined the "Z" area (Fig. 5). I demonstrated this
path over forty four years ago in the human anatomy dissection laboratory (Fig.
6,7). Last year, a striking unrehearsed event of monumental significance
took place in the medical examiner's office that confirms the existence of this
path. A young woman had been brutally stabbed over her whole body. I found a
defense wound on her hand where she had raised her hand in an attempt to protect
her face from the vicious onslaught. Examination of this wound in her hand
revealed that she was stabbed in the thenar furrow in the palm of the hand; the
knife had passed through the "Z" area and the point exited at the back of
the wrist exactly where it is displayed on the Shroud (Fig. 8).
X-rays of the area showed no evidence of broken bones!
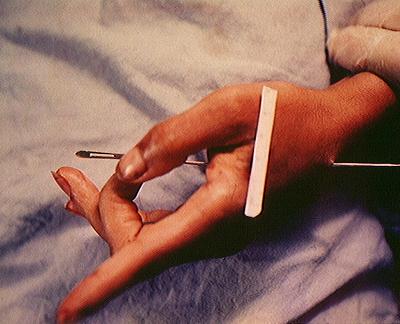
Figure 8
Although the radial side of the wrist cannot be excluded as a
possible pathway, the upper part of the palm is the most plausible location for
the following reasons:
- The palm region is the location most Christians across the
centuries perceived the wound to be.
- The path through the upper palm is very strong and
anatomically sound.
- The path ends exactly where the shroud shows the wound
image.
- In the ancient literature, Lipsius and other authors and
painters and sculptors related and depicted the hands that were transfixed in
crucifixion.
- It assures that no bones are broken in accord
with Exodus 12:46 and Numbers 9:12.
- It explains the apparent lengthening of the
fingers of the Turin Shroud because of nail compression at this area.
- Lastly, it is where most of the stigmatists( prior to Dr.
Barbet’s book ) like St. Francis of Assisi, Padre Pio, Theresa of Konnersruth,
St. Catherine of Sienna, Catherine of Ricci, Louise Lateau, etc. have displayed
their wounds throughout the centuries.
Hypothesis Two
The missing thumb on the Shroud was due to injury to the median nerve by the
passage of the nail. Barbet indicated that each time the nail was driven through
Destot's space, the median nerve was severed either halfway or two-thirds of the
way causing the thumb to be drawn into the palm. This of course is untenable
because as we demonstrated above, the median nerve does not pass through
Destot's space but runs along the opposite side (thumb or radial side) of the
wrist. Even if the median nerve was injured causing, mechanical stimulation as
Barbet claimed, this would still not cause the thumb to be drawn into the palm
of the hand. Dr. Ernest Lampe, one of world's leading hand surgeons who in
discussing injuries to the median nerve, relates in his book, Surgical
Anatomy of the Hand, that in severance of the median nerve...... "THERE
IS INABILITY TO FLEX THE THUMB, INDEX AND MIDDLE FINGERS". This was
confirmed to me by several hand reconstruction surgeons.
WHAT, THEN, WOULD ACCOUNT FOR THE MISSING THUMBS?
There is, however, a very simple explanation as to why the thumbs are not
visible on the Shroud. The thumbs are missing from the Shroud image because
their natural position both in death and in the living person is in the front of
and slightly to the side of the index finger. Therefore, it would be next to
impossible to have impressions of the thumbs because the Shroud would not be in
contact with them. You can demonstrate this by placing your arms and hands to
your sides and noting that the thumbs normally reside in front of the index
finger. Every day deceased individuals are brought into the Medical Examiners
Office, many of whom are transferred to our office from the local hospitals.
These usually arrive with their wrists crossed and tied together. In every case,
the thumbs are hidden in a position in front of and slightly to the side of the
index fingers.
Hypothesis Three
The Man of the Shroud died of asphyxiation. Asphyxiation is a physiological and
chemical state which results from an inability of a living organism to obtain
adequate oxygen for cell metabolism and to eliminate excess carbon dioxide.
Usually, a six to ten minute span of complete respiratory obstruction causes
irreversible brain damage and perhaps death. The asphyxiation or suffocation
theory was first propounded by LeBec in 1925 5, 6 and
Hynek in 1936.7, 8 It was, however, Barbet who refined it and
gave it its greatest impetus when he argued that three kinds of evidence all, a
priori supported his hypothesis:
The first evidence was the bifurcation pattern corresponding to the
image of the wound on the back of the hand. This was interpreted by Barbet as
representing two positions assumed by Jesus on the cross in order to expire
(breathe out). He postulated that Jesus was unable to expire in the lower
position and had to push up with his feet in order to expel the air from his
lungs. The interpretation of the bifurcation pattern is utterly absurd because
this pattern is located on the back of the hand-not on the front. Why
should that matter? Very simply, the back of the hand is pressed against the
patibulum of the cross by the nailing. How in the world can you get a perfect
double flow of blood? The heart is beating and is constantly extruding blood
through the wound and I assure the reader that the hand is heavily endowed with
blood vessels in vast networks constantly feeding from major blood vessels on
both sides of the hand. This would create a large blood smudge with blood all
over the hand, wrist and down the arm. This is supported by British Home Office
Pathologist James Cameron, a forensic pathologist who indicated that a nail
passing through the area of the median nerve would most likely hit a main
artery. Every movement on the cross would result in episodes of oozing and over
several hours there would be a substantial blood collection. Another important
point that militates against the two positions causing a "double flow of blood"
is the fact that the wrist does not change its angle even if the victim had to
raise himself in order to breathe. The reason-The arms bend at the elbows and
not at the wrists. We confirmed this during our suspension experiments
described below. An additional consideration derives from the excruciating pain
that would be experienced if the cruciarius attempted to raise himself by
putting an amount of pressure equal to the weight of the body against the nails.
Barbet's second evidence derived from the crucifragium or
skelokopia (breaking of the legs) of the two thieves (not Jesus), postulated
by Barbet as preventing the cruciarius from raising himself in order to
breathe. The reconstructions of the positions on the cross by both Haas9
and Zias and Sekeles10 from the Giv’at ha Mivtar
Excavation of the crucified 7 A.D. Jew, however, present evidence that the legs
were not broken to prevent the individual from lifting himself to breathe
because the body was already in a maximal, lifted position. Zias and Sekeles,
however, contend that Haas’ interpretation that the fractured tibia and fibula
bones were due to crurifragium is incorrect because the breaks are at
different angles and must have occurred after death. This interpretation does
not appear to be correct from a forensic point of view, because there may have
been more than one blow at different angles. The ritual of crurifragium (skelokopia)
was usually performed at a time when the victim was near death. This would be
the coup de grace blow which would hasten death by causing severe
traumatic shock in a person near death and in some instances, fatty embolism
could occur. Some authors have indicated that crurifragium was done to prevent
the victim from crawling away following removal from the cross so that wild
animals could devour their victims and Graves et al11 and
Seneca12 both indicated that crurifragium was also used as a
form of punishment. Barbet's third and last argument concerned the findings of
the Dachau concentration camp reports, where victims were suspended by their
wrists directly above their heads requiring them to raise themselves with their
hands in order to expire. Applying these observations to the asphyxiation
theory is like comparing apples to oranges. Here's why! When the hands and
arms are raised above the head to support the weight of the body, it is an
entirely different situation than that of a person suspended at an angle of
60-70 degrees with the stipes (upright). If Jesus was suspended with his hands
directly above his head, then there indeed, would be difficulty breathing but
not if the victim is suspended with his arms spread apart to create an angle of
65 to 70 degrees. Even Barbet concludes that Jesus was suspended at an angle
of about 70 degrees. This is also borne out on the photo of the cadaver he
suspended in his book Le cinq plait du Christ and on the crucifix
sculpted by Villandre1, 2 according to the specifications
given by Barbet. The results of Moedder's experiments are frequently used to
support the asphyxiation hypothesis but he suspended students by the wrists with
their hands above their heads and with the hands less than 40 inches apart on a
horizontal bail. It may be of interest to note that Dr. P.J. Smith disagreed
with Barbet's asphyxiation theory in appendix two of Barbet's own book.2
Experiments to Test the Validity of the Asphyxiation Theory.
The following experiments were designed with a view to determine whether the
asphyxiation theory is tenable or not.
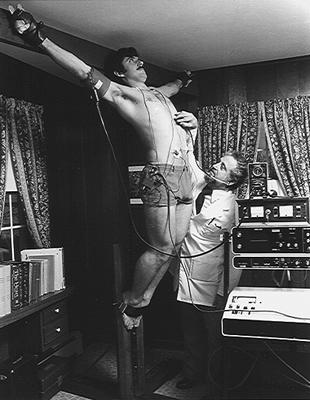
Figure 9
Experiment One
A very sturdy cross was constructed for me by the late Father Weyland, S.V.D.
with the stipes measuring 92" high and the patibulum measuring 3" wide and the
base secured with reinforced angle iron. A series of numbered holes were drilled
through each arm of the patibulum to allow for different arm lengths. This was
necessary because the longer the arm length the closer to vertical the
individual would hang if a single hole was provided for all arm lengths. Each
hole was drilled in a slightly downward direction from front to back so that the
bolts could be inserted from back to front in an upward direction to avoid
slippage by special leather gauntlets used to secure the hands to the patibulum
without constricting the wrists and compromising the blood supply. A hole was
provided on each gauntlet at the level of the base of the middle fingers so it
could be placed over the bolt that corresponded to the arm length of the
volunteer. Human volunteers between the ages of 20 and 35 were given a physical
examination and resting values were obtained which included, a 12 lead
electrocardiogram, pulse rate, blood pressure, auscultatory examination, vital
capacity and ear oximetry values, arterial blood gases, and venous blood
chemistries. A gauntlet was firmly tied on each hand and heart monitoring
electrodes were placed on their chests and attached to a stress testing
apparatus (Fig.9) which monitored the electrical patterns of the heart,
monitored the heart rate with digital readouts, and provided electrocardiogram
strips automatically, each minute. A blood pressure cuff with double transducers
was placed on the arm and attached to an Infrasonde electronic blood pressure
unit (Fig. 9) and a Water's ear oximeter probe was attached to an ear and
connected to an instrument that records the oxygen concentration of the blood at
all times. Each volunteer was instructed to inform us of any breathing
difficulties, pains of any kind, muscle cramps, or any other problems. They
were also requested not to attempt to lift the body up at any time by
straightening their legs. Each volunteer climbed up on a stool, placed their
outstretched arms along the patibulum to line up the holes in the gauntlets with
the respective holes on the patibulum corresponding to their arm length and
bolts were inserted into the appropriate holes through the back of the patibulum
then through the holes in the gauntlets. The stool was carefully removed
allowing the volunteer to be fully suspended (Fig. 9). A modified seat
belt was then utilized to secure the feet flush to the upright of the cross. An
emergency crash cart containing a defibrillator, cardiac medications and
intubation equipment was on hand to provide for the patients safety. Individuals
were stationed to the right and left of the volunteers in case of an emergency.
During the period of suspension, the following information was accrued and
tabulated: visual inspection was made for muscle twitching, chest excursions,
color, sweating, etc., and subjective information including pain, breathing
problems psychological feelings, etc. were also recorded. A heart-lung
evaluation including examination of heart and lungs with a stethoscope, periodic
arterial blood gases, ear oximeter readings, vital capacity, electrocardiograms
of specific leads, blood pressures, periodic blood chemistry screening including
a routine chemistry screen, CPK with isoenzymes, lactic acid, etc. Douglas bag
collections of the inspired and expired air were taken at various intervals.
Experiment Two
An experiment was performed on several of the volunteers who were requested to
push themselves up with their feet as was indicated in Barbet's Asphyxiation
Theory, in order to observe the angle of the wrist in both positions.
Experiment Three
Ten volunteers with angles of their arms with the upright between 60 to 65
degrees were studied by the above procedures but without strapping their feet to
the cross with the seat belt device to determine if the feet support had any
effect on breathing.
Results
- The volunteers were suspended for periods ranging from 5
to 45 minutes determined by when they wished to come down. The major reasons for
this decision was almost always due to the pain or cramping in the shoulders,
arms and hands.
- The angle of the arms with the upright varied between
individuals with a wide range from 60 to 70 degrees.
- There was no visual evidence of breathing difficulties
throughout the suspension.
- Subjectively, every volunteer affirmed that they had
absolutely no trouble breathing either during inspiration or expiration. A
common complaint was a feeling of chest rigidity and leg cramps between 10 and
20 minutes into suspension. When this occurred, they were allowed to straighten
their legs or come down.
- The oxygen content of the blood either increased or
remained constant. Both visual observations and Douglas bag studies determined
this to be the result of hyperventillation with abdominal breathing beginning
after 4 minutes at a rate about 4-5 times normal.
- Sweating varying in amount from mild to marked occurred at
about 6 minutes in most volunteers.
- The heart rate increased up to 120 at the end of their
suspensions but there were no arrhythmias. There were occasional rapid rates as
high as 175 but this decreased after the volunteer got over their initial
anxiety. The blood pressure increased to varying degrees but never above 160 mm,
systolic in everyone depending on their state of conditioning. The
electrocardiogram only showed muscle tremors and no cardiac abnormalities.
- The backs of the volunteers never touched the cross except
in the shoulder region of some volunteers where it was slight. Pain in
the shoulders caused many of them to arch their bodies back so that the top of
the head touched the stipes thereby relieving some of the pain .
- The Volunteers that were suspended without securing their
feet had no difficulty breathing but suffered a marked increase in pain in their
shoulders, arms and hands requiring the feet support or having to take them
down.
Cause of Death:
In order to arrive at the most probable cause of death, it is essential to
examine the sequence of all the events from Gethsemani through Calvary; the
severe mental anguish exhibited in the Garden of Gethsemani would cause some
loss in blood volume both from sweating and hematidrosis and provoke marked
weakness. The barbaric scourging that utilized a flagrum composed of leather
tails containing metal weights or bone at the tip would cause penetration of the
skin with trauma to the nerves, muscles and skin reducing the victim to an
exhausted, wretched condition with shivering, severe sweating, frequent displays
of seizures, and a craving for water. The results would cause a degree of
traumatic (injury) shock and hypovolemia (fluid loss), the latter resulting from
the sweating and the early stage of fluid accumulation around the lungs (pleural
effusion) from the effects of the scourging. Animal experimentation by Daniels
and Cate13 showed that blows to the chest in
animals resulted in rupture of the air spaces in the lung (alveoli) and spasms
of the air tubes (bronchi). Moreover the term "traumatic wet lung" refers to the
accumulation of blood, fluid and mucous from severe trauma (injury) to the
chest. The conclusion of traumatic shock from scourging, was also made by both
Tenney14 and Primrose.15 The irritation of
the trigeminal and greater occipital nerves of the scalp by the cap of thorns
from the Syrian Christ Thorn plant, Zizziphus spina christi especially
after he was struck several times with reeds would also contribute to traumatic
shock. The bumpy, uphill road to Golgotha in the hot sun, with the crosspiece on
the shoulder for a time, with falling some of the time, and being struck other
times also added to the hypovolemia and traumatic shock. The progression of the
pleural effusion would lead to increasing hypovolemia. The large square iron
nails driven through both hands into the cross would damage the sensory branches
of the median nerve resulting in one of the most exquisite pains ever
experienced by people and known medically as causalgia. The nails through the
feet would also elicit a great deal of pain. Both of these would cause
additional traumatic shock and hypovolemia. The hours on the cross, with
pressure of the weight of the body on the nails through the hands and feet would
cause episodes of excruciating agony every time the cruciarius moved.
These episodes and the unrelenting pains of the chest wall from the scourging
would greatly worsen the state of traumatic shock and the excessive sweating
induced by the ongoing trauma and by the hot sun, would cause an increasing
degree of hypovolemic shock.
The pathophysiological events that occur as a result of these events leading
to death are those of traumatic (injury) and hypovolemic (low blood and fluid
volume) shock. Shock, regardless of its cause is defined " ... as a
constellation of syndromes all characterized by low perfusion and circulatory
insufficiency, leading to an imbalance between the metabolic needs of vital
organs and the available blood flow.16 It is ".. a state of
inadequate perfusion of all cells and tissues, which at first leads to
reversible hypoxic injury, but if sufficiently protracted or grave, to
irreversible cell and organ injury and sometimes to the death of the patient.17
This presents a very complex array of initiating factors, compensatory reactions
and several interrelationships much too complex to include here. For an in depth
discussion of the mechanisms of shock invoked during crucifixion from initiation
to death please refer to my article, "Death by Crucifixion." 18
Conclusions:
- Destot's space does not conform to the hand image on
the Shroud of Turin. The hand wound image on the Shroud, is on the radial
(thumb) side of the wrist while Destot's space is on the ulnar (little finger)
side of the Wrist.
- Moreover the trunk of the median nerve could not be
severed if a nail passed through Destot's space because the median nerve is not
present in the area of Destot's space but instead runs along the opposite side
(radial) of the wrist in the thenar furrow into the Palm.
- The Shroud of Turin only shows the site of the nail's
exit and not where the nail entered. There are only two possibilities as to
where the nail entered: through the radial side of the wrist or through the
upper part of the palm angled toward the wrist.
- The most plausible region for the nail entry site in
the case of Jesus is the upper part of the palm since this area can easily
support the weight of the body, assures no bones are broken, marks the location
where most people believed it to be, accounts for where most of the stigmatists
have displayed their wounds and it is where artists through the centuries have
designated it and lastly it explains the apparent lengthening of the fingers of
the hand because of nail compression.
- The missing thumb on the Shroud image was not due to
injury to the median nerve by the passage of the nail. Injury to the median
nerve would not cause permanent flexion (bending of thumb into palm). Moreover,
the median nerve is not located in the area of Destot's space where Barbet drove
his nails.
- The thumbs are missing from the Shroud image because
the natural position both in death and in the living person is in front of and
slightly to the side of the index finger.
- The asphyxiation theory is completely untenable.
- The cause of death in crucifixion is a consequence of
shock.
REFERENCES
- P. BARBET, Les Cinq Plaies du Christ, 2nd
ed. Paris: Procure du Carmel de l'Action de Graces, 1937.
- P. BARBET, A Doctor at Calvary, New York:
P.J. Kennedy & Sons 1955; Image Books, 1963.
- A. PALEOTTO, Esplicatione del Sacro Lenzuolo Ove Fu
Involto il Signore, Bologna, 1599.
- E. W. Lampe, Surgical Anatomy of the Hand With
Special Reference to Infections and Trauma, Ciba Clin. Symposia 9:3-46,
1957.
- A. LEBEC, A Physiological Study of the Passion of
Our- Lord Jesus Christ, The Catholic Medical Guardian, 1925.
- A. LEBEC, Le Supplice de la Croix, I'Evangile dans la
vie, April, 1925.
- R.W. HYNEK, Science and the Holy Shroud,
Chicago: Benedictine Press, 1936.
- R. W. HYNEK, LeMartyre du Christ, 1937.
- N. HAAS, Anthropological Observations on the
Skeletal Remains from Givat ha Mivtar in Discoveries and Studies of Jerusalem
1970 Israel Exploration J.20:38-59, 1970.
- J. ZIAS and E. SEKELES, The Crucified Man from Giv'at
ha-Mivtar, Israel Explor. J. 35: 22-27, 1985.
- R. GRAVES and J. PODRO, The Nazarene Gospel Restored,
New York, Doubleday.
- SENECA, Ad Lucilius Epistulae morales. Epistle CL.
- R. A. JR. DANIELS and W. R .JR. CATE, Wet Lung-An
Experimental Study, Ann. Surg. 172:836,1948.
- S. M.TENNEY, On Death by Crucifixion, Amer. Heart
J. 68:286-287,1964.
- W.B. PRIMROSE, A Surgeon Looks at the Crucifixion,
The Hibbert J. 47:382-388, 1949.
- S. L. ROBINS and R. S. COTRAN, Pathologic Basis of
Disease, 2nd Edit. W.B. Saunders & Co. Phil. 1979, p. 112.
- S. L. ROBINS, R. S. COTRAN and V. KUMAR, Pathologic
Basis of Disease, 3rd Edit. W B. Saunders & Co. Phil. 1984, p. 138.
- F. T. ZUGIBE, Death by Crucifixion, Can.
Soc. For. Sci. J. 17:1-13, 1983.
|